Is grief a disease? Are some diseases invented and their importance exaggerated in order to increase the demand for drugs? Why did painkiller overdose cause the death of hundreds of thousands of Americans?
The pharmaceutical industry is sometimes accused of “making diseases” and deliberately medicalizing people. It's worth noting that during the COVID-19 pandemic, combined with the growing popularity of the anti-vaccine movement, writing about the "dark side" of the pharmaceutical industry is a little risky. Discussions about real abuses can easily be taken out of context and turned into yet another conspiracy theory against so-called Big Pharma.
But this is no reason to ignore the problems associated with the role of drug marketing in the spread of medicalization. Striving for evidence-based medicine rather than advertising bullshit, supporting unbiased scientific research, and adjusting pharmaceutical marketing strategies could restore trust in the pharmaceutical industry. Here we will try to understand what medicalization is, what it is like, and how pharmaceutical companies promote diseases to increase sales.
Medicalization and pharmaceuticalization
The concept of medicalization entered the literature of medical sociology in the 1970s to define the “participation of medicine in the governance of society.” One of the most succinct formulations comes from the American sociologist Peter Conrad: “defining a problem in medical terms, usually as a disease or disorder, or using medical intervention to treat it.”
Pharmaceuticalization is a term that ]]>denotes]]> “the process by which social, behavioral, or bodily conditions are treated or considered to require treatment or intervention with pharmaceuticals by physicians, patients, or both.” Sociologists have studied pharmaceuticals and the pharmaceutical industry for many years, but it was only in the 2000s that they developed a concept related to global political, economic and medical processes. The term “pharmaceutization” itself was introduced]]> into anthropology by Mark Nichter in 1989.
Historically, the concept of medicalization is associated with sociological criticism of medicine, considered as an institution of social control. Initially, medicalization was not a neutral concept, but rather a critical one, but over the years it has turned into a descriptive rather than an evaluative category. The emergence of the term “over-medicalization” shows that for many researchers, saying that something has been medicalized does not mean that it is wrong or wrong.
Numerous manifestations of medicalization include the replacement of various authorities by medical experts, the rethinking of certain forms of behavior previously considered, for example, sins, as diseases, an increase in the number of mental disorders, and an increase in the consumption of goods to maintain health. The last example should also be attributed to another sociological phenomenon - pharmaceuticalization. Pharmaceuticalization is understood as part of the consequences or as a subcategory of medicalization. This term describes a situation where something begins to be seen not only as a medical problem, but as a situation requiring the use of medications.
It is not surprising that effective marketing and advertising by the pharmaceutical industry to increase drug sales contributes to the spread of medicalization. Therefore, the pharmaceutical industry is one of the main factors pushing the medicalization of modern society.
The actions of drug companies accelerate the process of pharmaceuticalization, but are not its main or only cause. The pharmaceutical industry operates in an environment that is already medicalized. The relationship between Big Pharma and medicalization is more of a feedback loop than a one-way influence. Pharmaceutical marketing encourages a “cure-all” mentality, but the social reality that values health as a core value was not shaped by pharmaceutical companies.
QinetiQ, UK
The company was formed in 2001 when the UK Ministry of Defense split the Defense Evaluation and Research Agency (DERA) into two departments.
The first was called DSTL (Defense Science & Technology Laboratory). And the second part of DERA, responsible for most non-nuclear research, was renamed QinetiQ and prepared for privatization. It is now a public limited company (PLC) and has its headquarters in Farnborough in north-east Hampshire. It became one of the largest defense companies in the UK. In 2003, QinetiQ signed a long-term agreement (25 years) with the UK Ministry of Defense. And now the company supplies the British (and not only) army with innovative weapons, including robots.
TALON
is the name of a robotic platform that serves as the basis for creating robots for various purposes. They are called TALON family robots. In fact, the authors of the platform are Foster-Miller, which was acquired by QinetiQ. The manufacturer claims that this is one of the fastest platforms in production. It can move over rough terrain, overcoming water, snow, sand, and natural obstacles. Its weight can vary depending on the task performed: from 45 kg for combat missions to 27 kg for reconnaissance missions. The modular design allows TALON to be equipped with a variety of sensors, manipulators, tools and weapons. The company is now producing the fifth generation of robots on the TALON platform.
SWORDS
(Special Weapons Observation Reconnaissance Detection System) is the first robot from the TALON family to receive lethal weapons. Could be equipped with an M16 rifle, or an M249 SAW light machine gun of 5.56 mm caliber, or an M240 medium machine gun of 7.62 mm caliber, or a Barrett M82 semi-automatic rifle with a large-caliber 12.7 × 99 mm cartridge, or a six-barreled grenade launcher of 40 mm caliber, or a light four-barrel M202A1 FLASH 66mm flamethrower. In 2007, three examples with M249 machine guns were sent to Iraq, but were never used. After this, the US Army stopped funding robots and Foster-Miller created a different, more successful configuration - MAARS.
MAARS
(Modular Advanced Armed Robotic System) is a robot equipped with lethal weapons, which is designed for “reconnaissance, surveillance and target acquisition.” The first MAARS was shipped to the US Army in June 2008. The US Department of Defense immediately announced that any decision to use lethal weapons must come from the person who controls the robot. In the complete version, the robot was equipped with a number of cameras and sensors, an M240B machine gun with 450 rounds of 7.62 mm caliber and four M203 grenade launchers (could be loaded with various grenades, including smoke ones). The structure weighed about 167 kg. In some cases, the robot could be equipped with a loudspeaker, siren, laser blinding weapon and fire detection system. The MAARS battery lasted (depending on the intensity of use) for 3-12 hours.
Medicalization: pro et contra
An increasing number of human behaviors, characteristics or problems are viewed as medical rather than social, political, personal or religious issues. This can cause both positive and negative ]]>consequences]]>. The effects associated with over-medicalization are:
Because both the potential harms and benefits are significant, distinguishing between justifiable and harmful overmedicalization is critical. However, it's not that simple. There is an old and ongoing debate in sociology and philosophy of medicine about the correct definitions of disease and health. An alternative, pragmatic approach to this problem is that, rather than debating whether a condition is a true disease, ]]>should]]> carefully evaluate whether and why a particular condition should be included in the medical field of interest.
This approach is based on assessing and comparing the following points: the harm caused by the medicalized condition; adequacy, effectiveness and safety of medical decisions; the limits of social expectations regarding the normalization of individual behavior. That is, a comparison is made of the medicalization of a certain phenomenon with alternative ways of understanding it.
Meanwhile, it is the pharmaceutical industry that is actively involved in creating public and medical discourse about health. It is in the interests of the pharmaceutical industry that problems are perceived as medical and necessarily requiring the use of drugs. The industry influences the perception of certain problems and promotes its tools to solve them. Pharmaceutical marketing and drug advertising are sometimes even accused of “disease making” and making healthy people think they are sick. How justified are such accusations?
In the bioethical literature, this type of accusation is usually referred to as “disease trafficking” or “disease branding.” “Disease trading” can be ]]>described]]> as “expanding the diagnostic boundaries of a disease for reasons of economic gain.” Such “expansion” rarely involves literally creating or inventing new, unreal diseases. However, the pharmaceutical industry is willing to work hard to increase drug consumption, and some manipulations include changing our understanding of diseases in order to promote appropriate drugs.
The strategies of the “disease merchants” are conventionally divided into the following:
- medicalization of common conditions, as in the case of baldness;
- positioning mild symptoms as serious, such as irritable bowel syndrome;
- viewing personal or social problems as medical, as is the case with social phobia (only 12% of young people who described themselves as shy meet]]> criteria for social phobia);
- drawing up an idea of the risks as an independent disease, for example, osteoporosis ]]>suggest]]> treat before symptoms appear, using ]]>online calculator]]>;
- overestimating prevalence to maximize potential markets, as in the case of erectile dysfunction.
The above strategies seem reasonable, although the examples used will seem controversial to many. "Disease trafficking" is a real problem, but don't jump to conclusions like "there's no cure for osteoporosis" or "irritable bowel syndrome doesn't exist." This syndrome is known, but the benefits of most proposed treatment options ]]>weakly]]> have been proven.
Male pattern baldness ]]>is]]> physically benign, although it is increasingly being called a “disease” based on claims that it causes profound suffering. The over-medicalization of baldness, according to a meta-analysis of 37 studies, is supported by the fact that most studies were likely to have a commercial impact (78%), present baldness as a disease (77%), were conducted on biased samples (68%), and promoted products or services for growth hair (60%), overlooking restrictions (68%).
Psychologists ]]>believe]]> that it is necessary to fight the medicalization of baldness and allow men to make an informed choice whether to do something about their baldness or not. Thus, baldness is more of a cosmetic and aesthetic issue than a painful condition.
In the case of erectile dysfunction, which undoubtedly causes discomfort for men, normal medicalization has long gone to the highest, but not the best, degree, ]]>turning]]> into phallocentrism and ignoring the natural age-related decrease in libido or psycho-emotional causes that do not require medicinal intervention. This medicalization is promoted by urologists, the medical industry, the media and entrepreneurs. Despite the clear advantages it provides men, it has serious disadvantages - in terms of disappointment in the promised ideal erection and postulation of a false universalized and biologized vision of sexual experience.
At the same time, other sexual interests of women that differ from the phallocentric sexual scenario are denied. In addition, the artificially increased demand for drugs to improve erection ]]>stimulates]]> the supply of counterfeit drugs - 25% of such drugs in developing countries and up to 50% in some African and Asian regions, which often do not meet safety requirements, contain harmful chemical impurities and pathogenic bacteria. Some sources estimate the market for counterfeit erectile dysfunction drugs to be worth between $75 billion and $200 billion.
The medicalization of the female body and its natural processes is a separate and even more striking phenomenon. Today, premenstrual syndrome, menstruation, pregnancy, childbirth and menopause are practically equated to painful conditions. Also ]]>medicalized]]> sexuality, appearance and mood. Based on this, then being a woman is already a disease. Women are prescribed almost 70% of all medications and visit doctors four times more often than men. This makes women a key market for pharmaceutical companies throughout their lives.
Currently, a condition that is considered a disease or disorder is determined by various medical authorities through a complex assessment process. Development and revision of the International Statistical Classification of Diseases and Related Health Problems (ICD), or the Diagnostic and Statistical Manual of Mental Disorders (DSM) is a multi-year task involving scientific experts from all over the world. And mere conflict of interest or market pressure exerted on the assessment process is not enough to categorically deny these documents.
Promotion of diseases, for example by creating a marketing narrative about a condition and its prevalence, often occurs after the disease has been included in an official classification. Restless legs syndrome was for some time ]]>called]]> a fictitious or made-up disease, but began to be promoted many years after its introduction in ICD-9 to increase demand for drugs. However, to evaluate any instance of medicalization, one needs objective and reliable data on the specific disease, which is not always easy to obtain.
The pharmaceutical industry has many tools that, if used incorrectly, can distort the understanding of diseases and their treatments. These include sales representatives, drug marketing to physicians, direct advertising, Internet content, disease awareness campaigns, sponsored medical associations and patient communities, lobbying, astroturfing (feigning public support), targeted medical education, sponsored research, medical conferences and payment of medical experts - authoritative leaders of public opinion.
For the sake of profit, all of these tools are used to exaggerate the effectiveness and safety of drugs, encourage their unauthorized use (prescribing for off-label indications), lower thresholds for diagnosing diseases, or disseminate unverified data on the incidence of disease. As American researchers rightly noted, “one hand—the scientific divisions of the industry—works hard to discover new effective and safe drugs. Then the other hand—the marketing departments—turns good drugs into bad ones by expanding their actual use beyond the proper evidence base.”
Why do we need robotics competitions?
The founder of the Volnoe Delo Foundation, Oleg Deripaska, says that all the technology that surrounds us today was invented and created by engineers who had curiosity and a desire to learn the unknown. “What our future will be like depends on engineers and technical specialists. Their ideas, based on creativity, sound knowledge and a constant desire to innovate, move the world forward,” he believes.
The future of Russian and world robotics is now in the hands of children who are interested in this science, create their first projects, bring them to competitions to show their work and look at the experience of others.
“Children who cannot go to big competitions lose interest over time,” says Marina Kazakova, head of the robotics club at school No. 4 in the city of Pikalevo, Leningrad Region and federal judge of the AutoNet 10+ competition. “And when they participate in big competitions, they plunge into the environment and see other children and other projects. Including serious work by high school students. Those guys who were at all-Russian festivals no longer give up their places in the circle. In our country, places are released only by graduates or if new equipment appears and then we can take on new children.”
Here it is difficult to overestimate the contribution of the Robotics program of the Volnoye Delo Foundation, within the framework of which, since 2009, all-Russian engineering and technical competitions have been organized, which culminate with the all-Russian festival PROFEST (until 2017 it was called “Robofest”). PROFEST winners are already going to represent our country at international competitions. The head of the Volnoe Delo Foundation, Oleg Deripaska, believes that results are impossible without experience - development, training of the mind and talents:
“You have to look around, your breakthrough ideas are important. This is what develops future engineers in you.”
Currently, more than 15 thousand schoolchildren and students from 69 regions of Russia participate in the Robotics program. In more than ten years, 500 regional resource centers have been created and more than a thousand certified instructors have been trained. 27 universities and 8 partner enterprises cooperate with the program.
The largest universities in Russia where participants of the Robotics program competitions study:
- Moscow State University named after. M. V. Lomonosova; Moscow Institute of Physics and Technology;
- Moscow State University named after. N. E. Bauman;
- Novosibirsk State University named after. R. E. Alekseeva;
- Irkutsk State University.
During the existence of the program, more than 100 thousand schoolchildren participated in the PROFEST festival. Every third of them subsequently entered a technical university.
“Current specialists in the field of robotics grow from creative associations, schools and institutions of additional education,” says Alena Asiatseva. “When a child becomes interested from an early age, tries it, understands what it is, then he consciously makes a choice towards a profession. And in the end, such children turn out to be cool specialists. Many guys, even at the stage of additional education, create systems that are then implemented in different areas.”
Anastasia Siginova remembers her students at children's competitions, whom she met years later in Skolkovo at competitions to create an autonomous driverless car, as part of teams of large companies, or as students of robotics departments. “It’s very nice,” she shares.
Medicalization of grief
The historian and philosopher ]]>Ivan Illich]]>, one of the first social critics of modern medicine, in the book “]]>Nemesis of Medicine]]>” unequivocally condemned the general idea of the medicalization of pain. According to him, by viewing pain only as a medical problem, we are trying in vain to avoid the fact that suffering is an inevitable part of human existence. In the past, communities had different cultural, religious, and philosophical ideas about the role of pain in life. Nowadays, thanks to the medicalization of pain, any suffering has become useless and meaningless, and the only weapon against it is painkillers.
Illich's arguments are quite controversial, and according to the pragmatic approach to medicalization, in the case of physical pain it is quite justified because:
1) pain causes harm;
2) recognizing physical pain as a problem is not an example of unjustifiably restricting the diversity of individuals for the sake of normalization;
3) medicine provides the most adequate methods for understanding physical pain and its causes;
4) medicalization of pain provides the most effective and safe methods of alleviating suffering.
Therefore, in general, the medicalization of physical pain can serve as an example of good medicalization. However, this does not mean that every medical or pharmaceutical response to every type of mental suffering will be equally justified.
On the other hand, the medicalization of grief, especially when only a short duration of grief is seen as normal, is sometimes considered an example of over-medicalization. According to DSM-IV, bereaved people were only eligible for a diagnosis of major depressive disorder if symptoms were “excessively severe or prolonged,” with duration defined as “more than two months after the death of a loved one.” person>". In the DSM-IV, what is called prolonged grief disorder or persistent complex bereavement disorder was recognized as a separate mental condition.
However, limiting long-term depression after the death of a loved one to lasting more than two months is controversial. Today, long-term grief disorder is not recognized as a distinct mental health condition with clear diagnostic criteria. The eleventh revision of the International Classification of Diseases (ICD-11), which comes into force in January 2022, sets a threshold of six months for confirming a diagnosis of depression, which clearly exceeds the expected cultural, social or religious norms found in specific culture and context, and in ]]>DSM-V]]> - two months.
The medicalization of normal grief ]]>stigmatizes]]> and diminishes the normality and dignity of pain, distorts the intended existential processing of loss, and exposes many people to unnecessary and potentially harmful drug treatment.
Diagnosing depression in situations where a person is experiencing grief can easily become a push and serve to promote appropriate medications. People who treat depression with antidepressants are more likely to have ]]>depressive episodes in the future than those who take no medication at all, a meta-analysis of nearly 40 years of published studies has found.
Patients with major depressive disorder who do not take medication have a 25% risk of relapse, while those who use antidepressants and then stop taking them have a 42% risk of relapse. This creates a vicious circle of cycles of prescription and withdrawal of drugs. The question arises: does it make sense to prescribe drugs to those who do not need them and involve them in this cycle?
Proponents of the medicalization of grief ]]>agree]]> that there have been no ideal studies defining the full spectrum of normal depression and clear boundaries of this condition. Experts say the harm that could occur if ordinary grief is overdiagnosed as MDD pales in comparison to the harm of missing a diagnosis of major depression. Given that completed suicide occurs on average in about 4% of patients with MDD, much greater harm would be done to patients if clinicians were encouraged to exclude from the MDD category those who developed major depressive symptoms within two months of bereavement. A counter-accusation to opponents of medicalization is the “normalization” of the disease.
Demedicalizing grief does not mean that people who mourn for long periods of time should not take antidepressants at all. However, the medicalization of bereavement in the light of a pragmatic approach is considered controversial because the causes of grief-related suffering are not medical, and establishing a time frame for “normal” grief can be seen as over-standardizing and pathologizing individual experiences.
Use of Russian robots
In Russia, robots are still rarely used. But there is a trend towards robotization of production in various fields of activity.
Robotic systems for ship repair
The Ministry of Industry and Trade plans to use robots to increase labor productivity during ship repairs by 2–3 times. Shipbuilders will soon receive mobile container systems that are equipped with lasers.
The use of such systems will significantly reduce repair costs and vessel downtime. The main purpose of their use is to improve the operational safety of offshore facilities and to control damage.
The prototype of the system will include two containers: laboratory-transport and technological. They will house equipment intended for laser cladding, restoration of anti-corrosion coatings, and repair of the anchor system.
Robot manipulator in the form of a hand
In Russia, hand-shaped manipulators are produced only by Aripix Robotics. They are gradually being introduced into production facilities built like a conveyor belt. Such a robot can perform various operations, as it has 6 axes. But it is mainly used for packaging goods.
Garbage sorting robot
Moskovskaya has created the first domestic robot that can automatically sort garbage. The device has a scanner that determines the type of waste. The robot recognizes 20 types of plastic, analyzes color, chemical composition, etc. The device can process about 130 objects in a minute.
Robot Fedor
Robot Fedor or Skybot F-850 was created by Evgeny Dudorov specifically to perform work in space. In 2022, the device was sent to the ISS, where it successfully passed all tests. A few days later the device was returned to Earth.
Androids from Promobot
An unusual employee appeared in one of the Perm MFCs - a humanoid robot, which was developed by the Promobot company. He works full time. The device has been tested and proven to be highly effective.
The robot's task is to consult clients. He is able to help people fill out documents and answer many questions. In the near future it is planned to add a function for accepting payments.
The figures confirm that the Russian robotics market is actively developing. But the actual use of robots in Russia is very low. To accelerate the development of the industry, it is necessary that the state pay attention to it, since the public sector is the most backward in technical terms.
- December 20, 2020
- 508
Exoskeleton ExoAtlet Albert, LLC ExoAtlet, Russia
Medical exoskeleton, the second version of the ExoAtlet exoskeleton, developed in 2014. The expected cost of the first commercial copies is 1.5 million rubles. Designed for paraplegics; in addition, modifications of the exoskeleton are being developed for patients with other diseases.
In July 2016, the collection of pre-orders for the purchase of the exoskeleton began.
JSC "Plant named after. V.A. Degtyareva", Russia
Construction of the plant began on August 27, 1916 in Kovrov (Vladimir region). The plant was among the first to receive a license to produce the Madsen submachine gun. After the October Revolution, the Danish part of the administration tried to dismantle and remove the equipment, but the plant workers did not allow this to be done. In 1918, the plant was temporarily closed due to lack of money. But already in July 1919 it was nationalized, and by 1920 it employed more than 1 thousand workers. It was called “Kovrov Machine Gun Plant”, “Tool Plant No. 2 named after K.O. Kirkizh", and in 1949 the enterprise was renamed the plant named after V.A. Degtyareva. In 1940, he began producing the legendary PPSh. And with the beginning of the Great Patriotic War, the plant switched to round-the-clock operation. Now it produces weapons, motorcycles, industrial sewing machines, batteries and equipment for the food industry.
"Nerekhta"
- a combat robotic complex developed on behalf of the Foundation for Advanced Research (Russian analogue of DARPA). The robot's platform is modular, thanks to which it can be turned into a combat, reconnaissance or transport vehicle. In combat equipment it is equipped with a 12.7 mm Kord heavy machine gun or a 7.62 mm Kalashnikov tank machine gun (PKT), as well as an AG-30M automatic grenade launcher system of 30 mm caliber. It is also possible to install the Kornet anti-tank missile system. Equipped with laser video cameras, laser rangefinder, thermal imaging camera. The maximum target detection range with a combat module is 3000 m. With an artillery reconnaissance module - 5000 m. The effective target engagement range is 1000 m. It moves on caterpillar tracks at a speed of up to 32 km/h. Platform weight without modules is 1000 kg, load capacity is 500 kg. The robot's armor can withstand a 7.62 mm caliber bullet fired from a sniper rifle or machine gun (protection class - 5). The version with a transport module is equipped with a manipulator, a coupling device, a winch with a trawl and a transport container.
Endeavor Robotics, USA
A team of engineers and developers who previously worked for iRobot (discussed in the second part of the review of military robots). It still produces devices such as Firstlook and Packbot, but it also has its own separate development - Kobra.
Kobra
is a robot minesweeper. With its own weight of 226.7 kg, the robot is capable of lifting objects weighing 150 kg when folded and 35 kg when fully extended. The coverage radius of the manipulator is 190.5 cm. The robot is equipped with four cameras and can reach speeds of up to 12.9 km/h. However, it can move on surfaces with an impressively large slope of 55 degrees. Can work autonomously for up to 10 hours straight.
While politicians argue
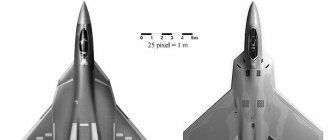
Today, enterprises of the Russian defense complex are developing ground combat robots of the Uran, Nerekhta and Soratnik families, which are planned to be used for fire support of infantry, protection of military and important infrastructure facilities, reconnaissance in force, and breakthrough of enemy defenses. In turn, in the United States, work is underway to create XQ-58A Valkyrie unmanned aerial vehicles, which would serve as wingmen in fighter combat groups. Such drones could conduct reconnaissance, cover a manned lead fighter, conduct maneuverable air combat, or provide airborne fire support to ground troops.
South Korea is developing reconnaissance and combat air, ground, surface and underwater robots that would help compensate for the shortfall in the armed forces. China, among other things, is working on robotic tanks that will reduce losses in intense tank battles. And in Israel, in the next few years, it is planned to adopt combat microrobots that will be used to destroy the leaders of the Hezbollah and Hamas militants.
The ethical and legal aspects of such developments require careful discussion. Is it possible to give robots the right to kill people? Is it acceptable to replace people who are able to feel a particular situation with emotionless performers? Where is the line between civilian and military developments of autonomous robots, which are based on the same technologies? Is it right to remove soldiers from the battlefield and seat them at control panels with comfortable chairs thousands of kilometers away from the fighting?
“Killer robots” have not yet become part of modern warfare, but we should start preparing the legal framework for the use of such systems now, because progress is moving very quickly. Both the United States and Russia and some other countries say that they do not plan to make combat systems completely independent. At the same time, the United States noted that they allow the possibility of switching “killer robots” to a fully autonomous mode as a response to the emergence of combat autonomous robots in authoritarian regimes.
Vasily Sychev